Recurrent Shoulder Dislocation and Coracohumeral Ligament Tear: Beyond Bankart and Hill–Sachs
Clinical Presentation
A 29-year-old male presented with recurrent anterior shoulder dislocation. The patient reported multiple episodes of instability following an initial traumatic dislocation. Physical examination revealed anterior shoulder pain and apprehension with external rotation.
Imaging Findings
1. Glenohumeral Instability Lesions
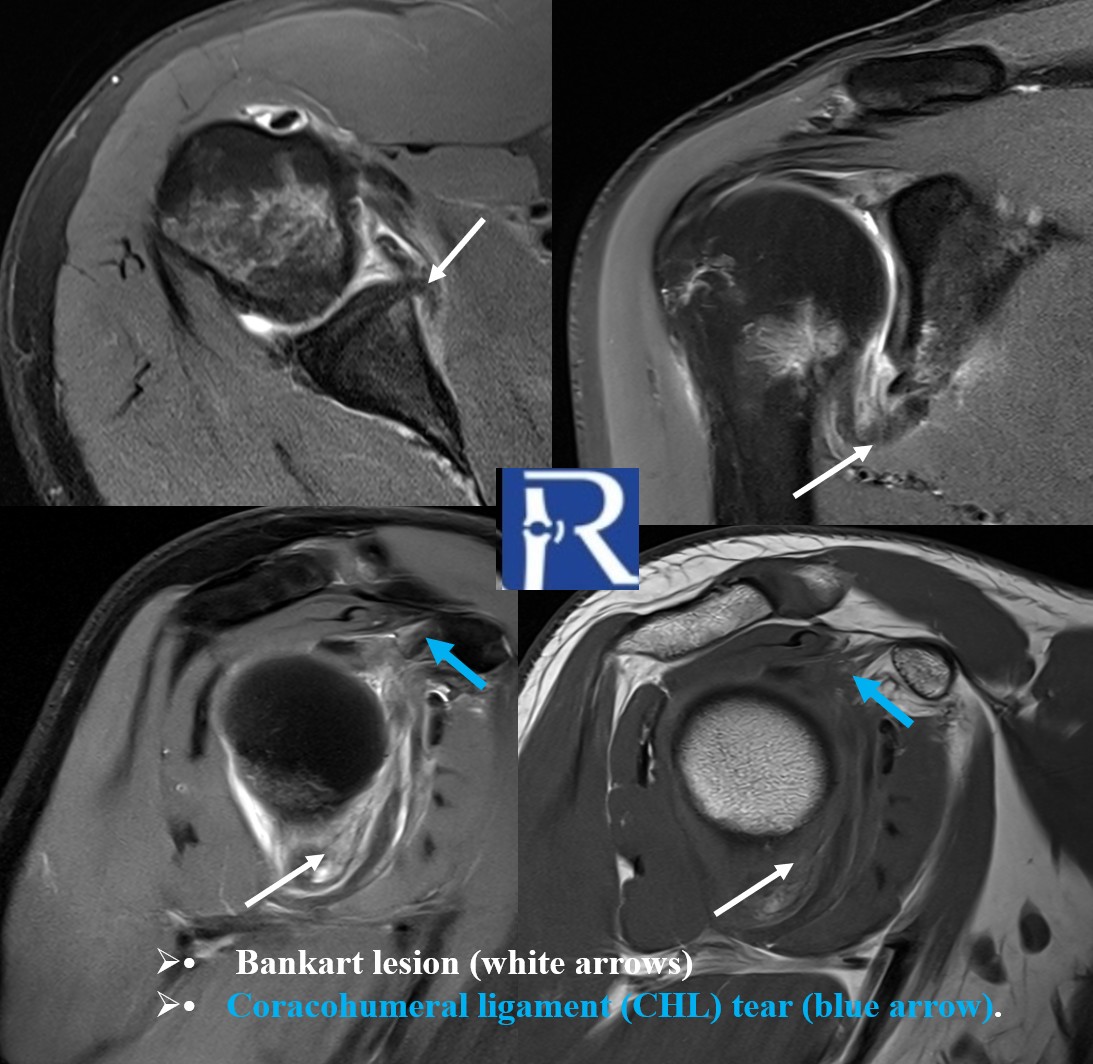
- Posterior cortical impaction fracture of the humeral head, consistent with a Hill–Sachs lesion (white arrows).
- Avulsion of the anteroinferior labroligamentous complex at the glenoid rim, consistent with a Bankart lesion (white arrows).
- Adjacent contusional bone marrow edema seen around both lesions.


2. Anterosuperior Capsuloligamentous Injuries
- Coracohumeral ligament (CHL) tear (blue arrow).
- Superior glenohumeral ligament (SGHL) tear (yellow arrow).
- Middle glenohumeral ligament (MGHL) tear (red arrow).


These findings highlight injury to the biceps pulley system components and rotator interval stabilizers that are often overlooked on routine shoulder MRI.
Discussion
While Bankart and Hill–Sachs lesions are well-recognized contributors to anteroinferior shoulder instability, this case emphasizes additional anterosuperior stabilizers that are critical for glenohumeral joint integrity:
- The coracohumeral ligament (CHL) is a pivotal element of the biceps pulley system and a major stabilizer of the rotator interval.
- The superior glenohumeral ligament (SGHL) also contributes to the pulley mechanism and humeral head stabilization, particularly in early external rotation and overhead positions.
- Injuries to these structures may predispose to anterosuperior instability, which is not routinely assessed in standard reports.
Routine shoulder MRI interpretation should therefore include careful assessment of the CHL, SGHL, and MGHL, especially in cases of recurrent instability, because they play a substantial role in maintaining anterosuperior shoulder stability and biceps tendon stability.
Key Teaching Points
- Bankart and Hill–Sachs lesions explain anteroinferior instability, but may not account for all instability patterns.
- The coracohumeral ligament (CHL) is a key stabilizer of the rotator interval and a major component of the biceps pulley system.
- Superior glenohumeral ligament (SGHL) injury frequently accompanies CHL tears and contributes to anterosuperior instability.
- Middle glenohumeral ligament (MGHL) tears further weaken capsuloligamentous support.
- Routine shoulder MRI interpretation should include systematic evaluation of CHL and SGHL, structures that are often overlooked.

0 COMMENTS
These issues are no comments yet. Write the first comment...