Humerus
Medullary Osteonecrosis of the Proximal Humerus

Clinical History
A 60-year-old woman presented with right shoulder pain, progressively worsening over months. Her medical history is significant for intermittent corticosteroid use over several years for various conditions. No recent trauma was reported.
Imaging Findings
Radiography (Two Views)
- There is a medullary lesion involving the proximal metaphysis and diaphysis of the right humerus.
- The lesion displays a mixed lytic and sclerotic pattern with irregular margins within the medullary cavity.

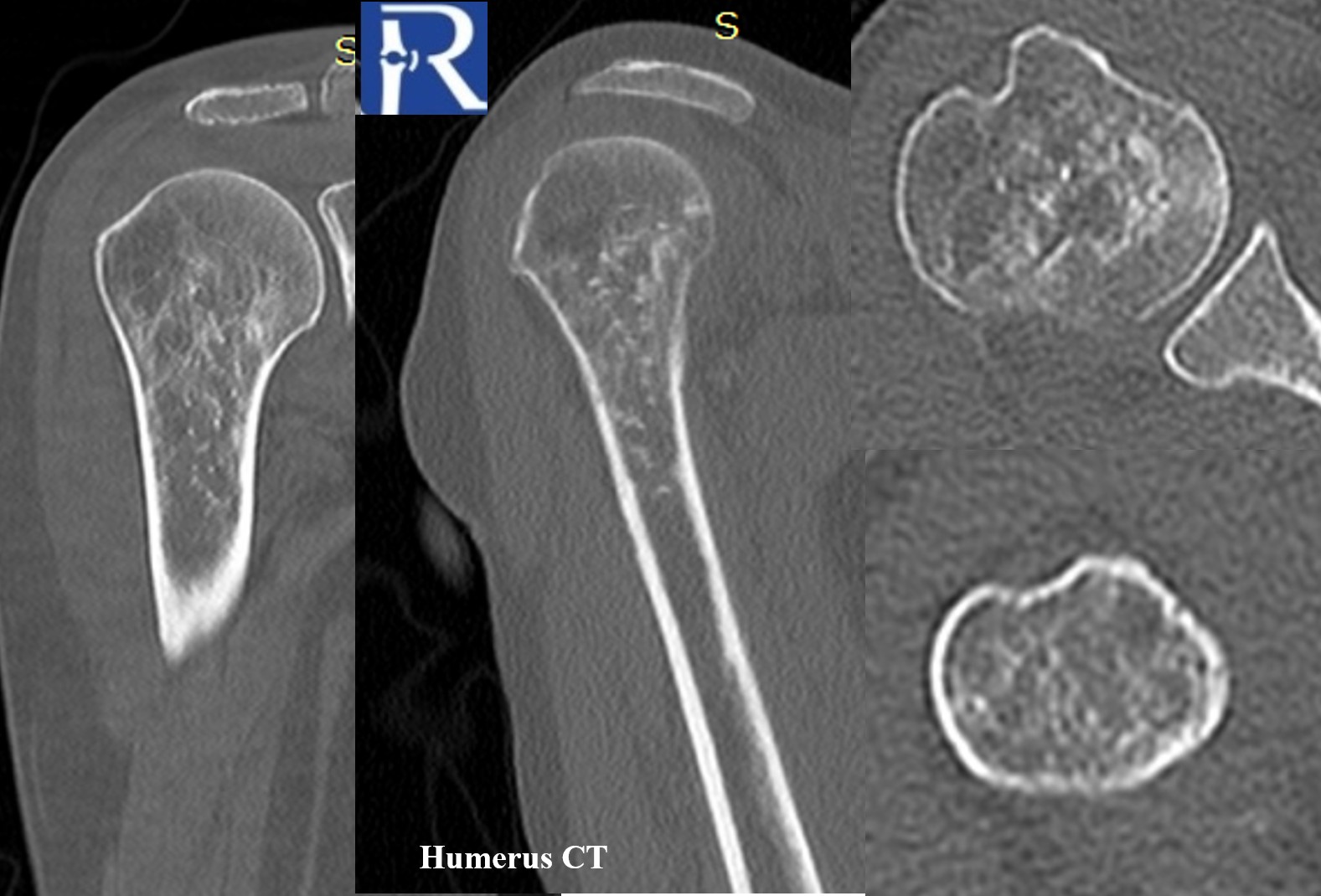
Computed Tomography (CT)
- The lesion is more clearly delineated on CT, showing multiple tiny punctate calcifications embedded within the lesion.
- These punctate densities are suggestive of a chondroid-type matrix, though non-specific.
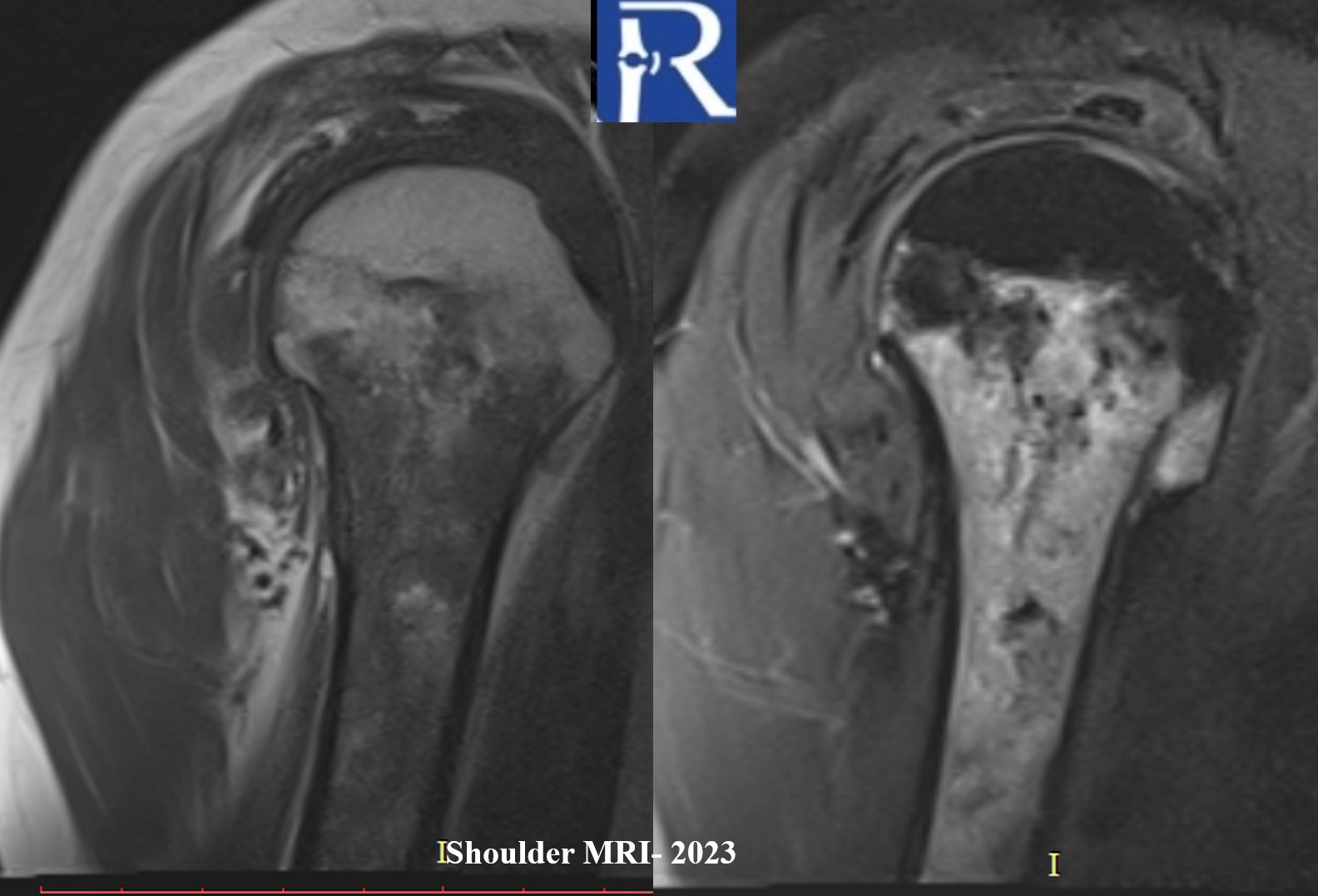
Magnetic Resonance Imaging (MRI)
- Retrospective review of a 2023 MRI revealed ill-defined heterogeneous bone marrow signal abnormalities consistent with bone marrow edema-like changes in the same region.
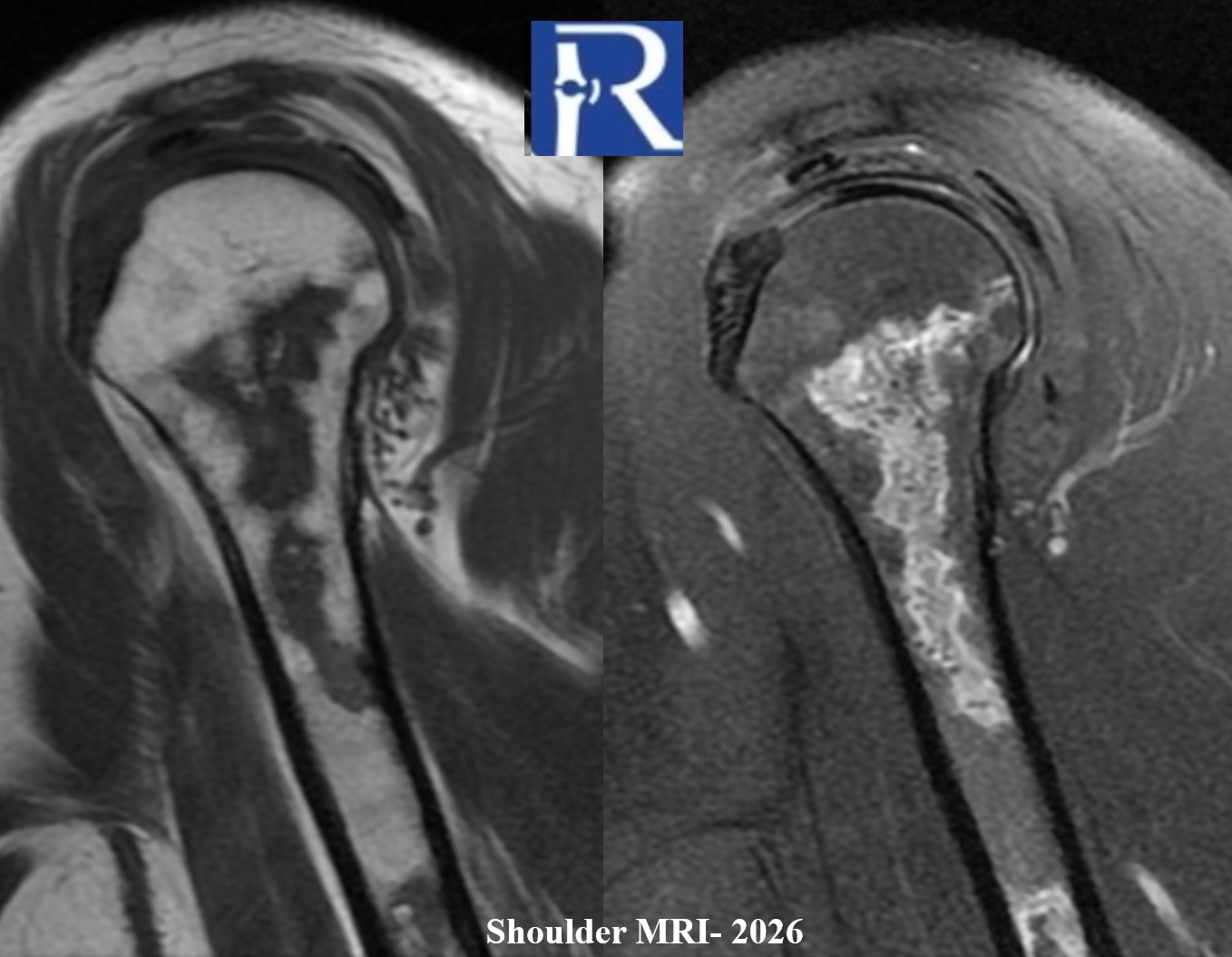
- Current MRI demonstrates a better defined medullary lesion with a geographic pattern and signal characteristics in keeping with medullary osteonecrosis.
Differential Diagnosis
Primary considerations include:
- Medullary osteonecrosis (bone infarct) – favored by the history of steroid use and imaging evolution.
- Chondroid neoplasm (e.g., enchondroma or low-grade chondrosarcoma) – considered due to the punctate calcifications but less likely given temporal imaging and clinical context.
- Bone metastasis – less likely without known primary.
- Other benign marrow processes (e.g., atypical bone marrow edema syndromes).
- Discussion
- Osteonecrosis refers to ischemic death of bone and marrow components, and can affect various bones, especially in the setting of corticosteroid exposure. The imaging appearance of medullary osteonecrosis commonly includes a serpiginous sclerotic margin on radiographs; however, these findings are not always classic or pathognomonic.
- In this case, serial imaging shows evolution from ill-defined marrow signal change to a geographically delineated medullary lesion, supporting the diagnosis of steroid-associated medullary osteonecrosis rather than a neoplastic process. CT adds value by demonstrating peripheral or matrix mineralization, which may be observed in chronic osteonecrotic lesions
Teaching Points
- Clinical context (e.g., steroid use) is critical when interpreting mixed lytic–sclerotic medullary lesions.
- Multimodality imaging (XR → CT → MRI) enhances diagnostic confidence, particularly in distinguishing ischemic necrosis from neoplasia.
- Temporal progression of findings contributes valuable diagnostic insight, especially when prior imaging is available.
- CT can better demonstrate fine mineralization patterns within marrow lesions not well seen on radiographs.

0 COMMENTS
These issues are no comments yet. Write the first comment...