Long-Term Sequelae of Childhood Rickets Manifesting as Patellofemoral Instability in Adulthood: A 15-Year Imaging Follow-Up

Long-Term Sequelae of Childhood Rickets Manifesting as Patellofemoral Instability in Adulthood: A 15-Year Imaging Follow-Up
Miran Nihal Otlu, Aslı Irmak Akdogan, Ozgur Tosun
* Department of Radiology, Izmir Katip Celebi University, Ataturk Training and Research Hospital, Izmir/Turkey
Abstract
We present the case of a 25-year-old woman with bilateral knee pain, progressive lower-extremity malalignment, and recurrent lateral patellar dislocation, in whom serial imaging spanning 15 years documents the natural history of nutritional/metabolic rickets sequelae despite early corrective surgery. Initial radiographs at age 11 demonstrated classic active rachitic changes with severe genu valgum and femoral diaphyseal bowing. Three years after bilateral distal femoral corrective osteotomy with plate fixation, residual valgus alignment persisted. At skeletal maturity, full-length standing radiographs, CT, and MRI demonstrated persistent mechanical-axis deviation, trochlear dysplasia, markedly elevated tibial tubercle–trochlear groove (TT–TG) distance, and bilateral fixed lateral patellar dislocation. This case illustrates that incompletely corrected metaphyseal–diaphyseal deformity from childhood rickets can drive the development of secondary trochlear dysplasia and disabling patellofemoral instability years after physeal closure, and underscores the value of long-term radiographic surveillance in this population.
Introduction
Nutritional and hypophosphatemic rickets remain important causes of pediatric lower-extremity malalignment. The hallmark radiographic findings in the active phase — metaphyseal widening, cupping, fraying, and physeal indistinctness — are well described, as are the residual deformities of genu valgum or varum, diaphyseal bowing, and short stature. The patellofemoral consequences of these sequelae, however, are comparatively under-emphasized in the literature. Persistent valgus mechanical-axis deviation, distal femoral torsional abnormality, and a laterally displaced extensor mechanism may, over time, generate a maladaptive trochlea and chronic patellar maltracking. We present a case in which serial imaging across childhood, adolescence, and adulthood documents this trajectory, providing a clinicoradiologic illustration of how a pediatric metabolic disease may produce a patellofemoral problem in the third decade of life.
Case Report
Clinical history
A 25-year-old woman presented with a several-year history of progressive bilateral anterior knee pain, episodes of patellar giving-way, and a perceived worsening of her lower-extremity alignment. Her past medical history was notable for nutritional rickets diagnosed in childhood and bilateral distal femoral corrective osteotomies with internal fixation performed at the age of 14 for severe genu valgum. There was no history of major trauma. Examination revealed persistent bilateral valgus alignment, a positive J-sign on active knee extension, apprehension on lateral patellar translation, and full but painful range of motion. Laboratory parameters of calcium-phosphate metabolism were within normal limits at presentation.
Imaging findings
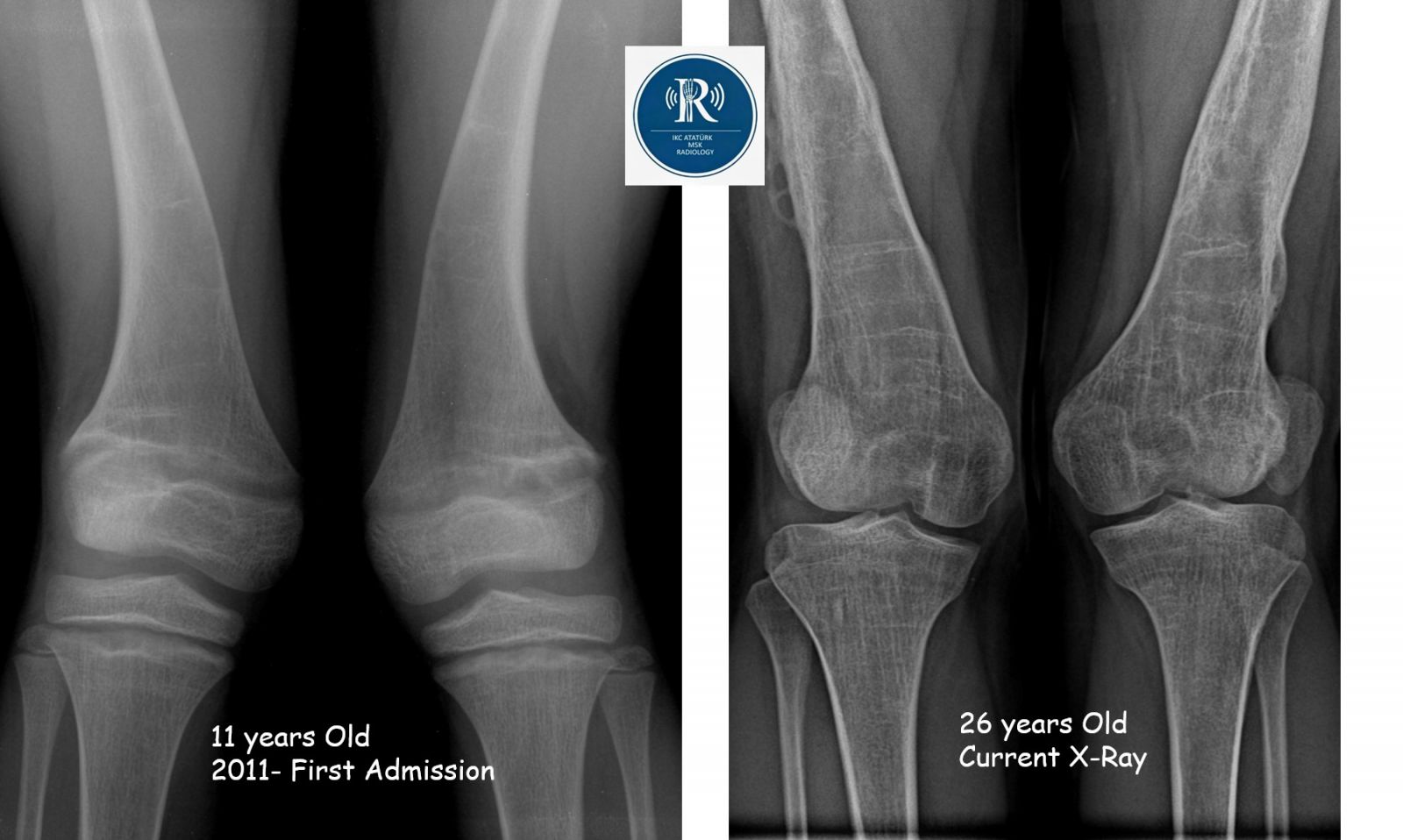
Index radiographs (2011, age 11). Standing antero-posterior radiographs of the lower extremities demonstrated marked bilateral genu valgum with the mechanical axis projecting well lateral to the lateral tibial spine. Both distal femoral metaphyses showed widening, cupping, and irregular fraying of the zone of provisional calcification, with indistinct, broadened physes — classic findings of active rickets. Diaphyseal bowing of both femurs was evident. Multiple transverse, sclerotic Harris growth-arrest lines were present in the metaphyses, indicating prior episodes of temporary growth deceleration.
Postoperative radiographs (2014, age 14). Bilateral distal femoral plate-and-screw constructs were in situ following corrective osteotomy. The mechanical-axis deviation was reduced but not fully neutralized; residual valgus and diaphyseal femoral bowing persisted. The rachitic metaphyseal changes had largely resolved, in keeping with adequate medical therapy.
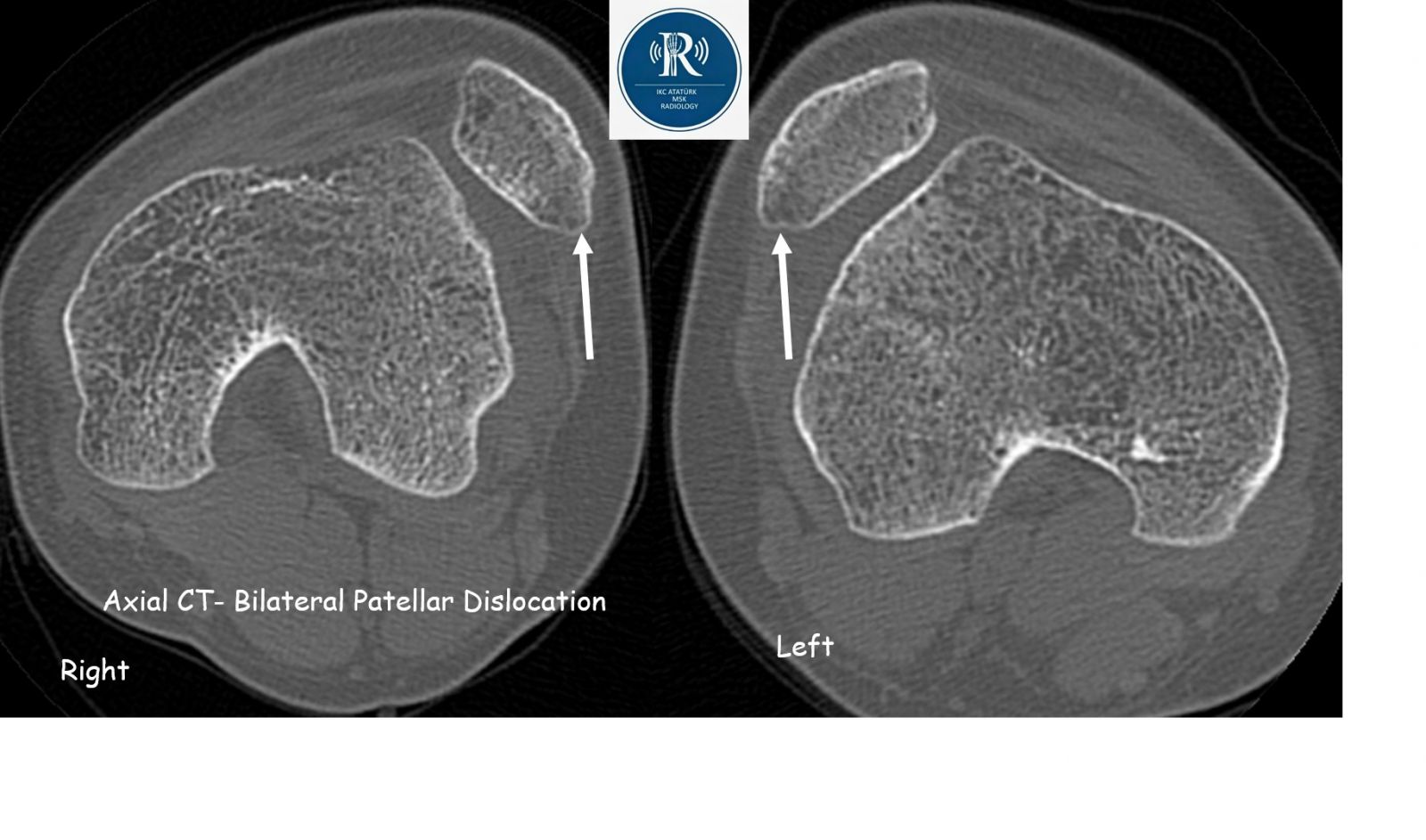
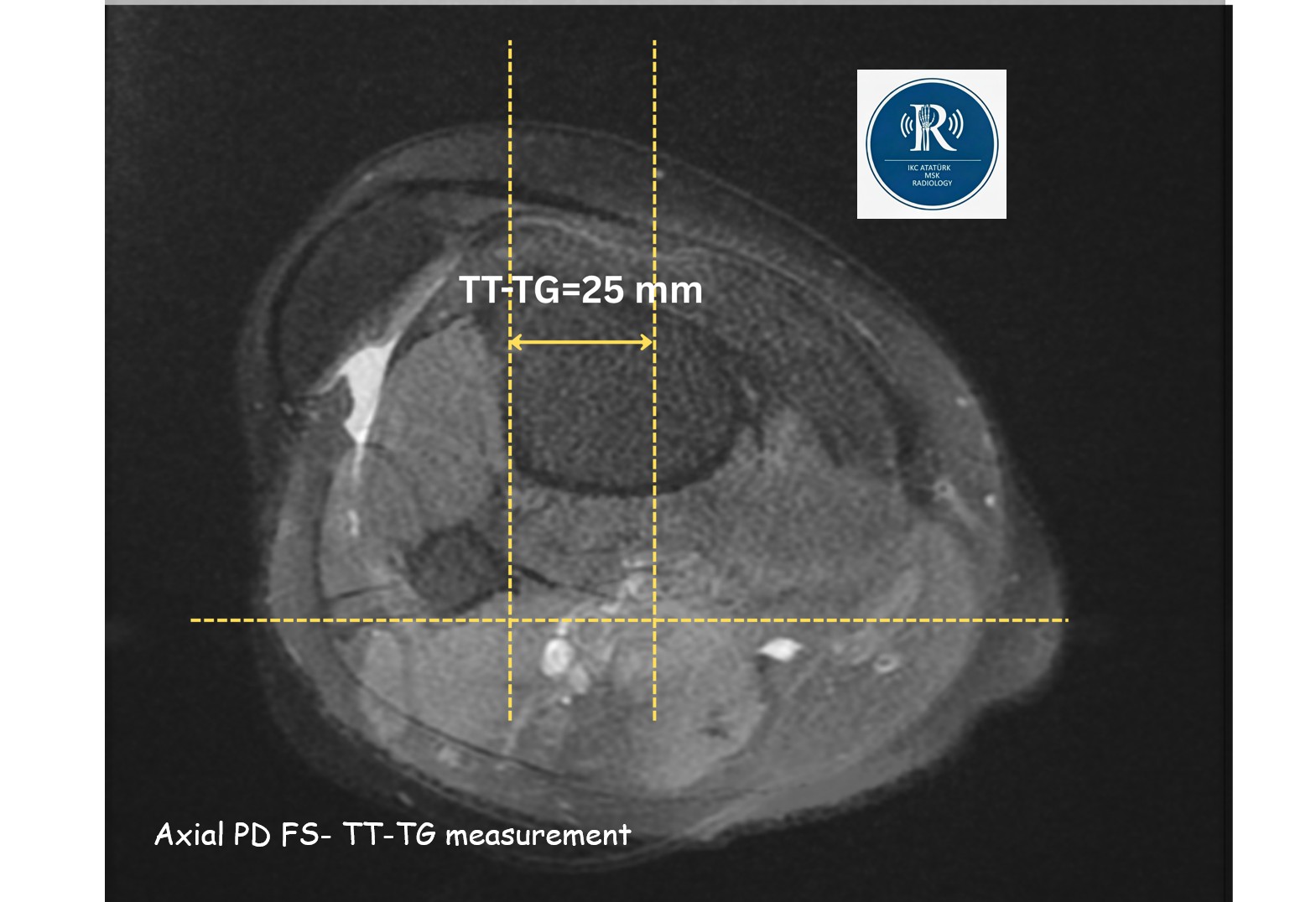
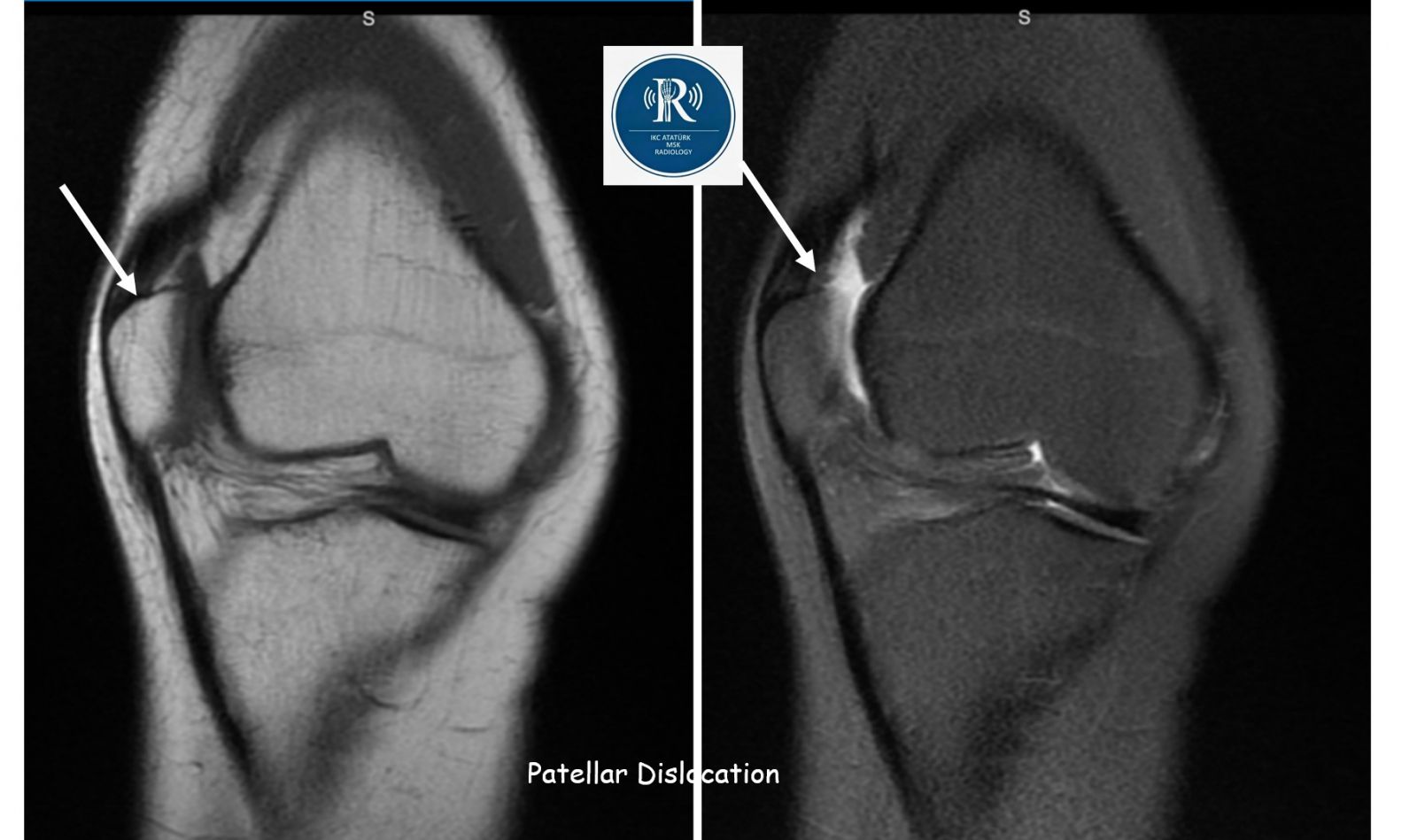
Current imaging (2026, age 26). Full-length standing radiographs demonstrated bilateral residual genu valgum with persistent femoral diaphyseal bowing and a laterally deviated mechanical axis. Harris lines remained visible as fine sclerotic bands perpendicular to the cortex within both distal femora and proximal tibiae, accompanied by linear trabecular sclerosis along the previous screw tracks following hardware removal. CT examination demonstrated a shallow, dome-shaped trochlea with diminished sulcus depth and a convex anterior trochlear contour consistent with trochlear dysplasia, together with a markedly elevated TT–TG distance bilaterally. MRI confirmed bilateral fixed lateral patellar dislocation with attenuation of the medial patellofemoral ligament, full-thickness chondral fissuring along the median ridge of the patella, and trochlear cartilage thinning at the lateral facet. No acute osseous injury or marrow edema indicative of recent trauma was identified.


Discussion
This case crystallizes a clinically important but under-recognized trajectory: a pediatric metabolic bone disease producing, decades later, a structural patellofemoral problem. Several features warrant emphasis.
First, the index radiographs display the textbook active phase of rickets — metaphyseal cupping, fraying, and physeal widening with mechanical-axis deviation — alongside features that are themselves a chronicle of past disease activity. Harris lines, the transverse sclerotic bands oriented perpendicular to the long-bone cortex, record episodes of transient growth slowing followed by resumption of normal endochondral ossification. Their persistence into adulthood in this patient, decades after metabolic stabilization, is a durable radiographic fingerprint of the childhood illness. The linear trabecular sclerosis tracking the prior screw paths is a separate, surgically induced finding and should not be mistaken for further growth-arrest phenomena or a sclerosing bone dysplasia.
Second, despite anatomically reasonable corrective osteotomies performed at age 14, the mechanical axis was not fully restored, and femoral diaphyseal bowing — a deformity that is intrinsically diaphyseal rather than physeal — was not addressed. Distal femoral osteotomy alone may be insufficient when the apex of deformity lies in the diaphysis, a recognized pitfall in the surgical planning of rachitic limbs. The residual valgus, compounded by likely distal femoral antetorsion that often accompanies the rachitic distal femur, predisposes to a laterally directed extensor-mechanism vector across the developing knee.
Third, and central to this presentation, is the link between long-standing malalignment and the development of trochlear dysplasia. A growing body of evidence supports the view that the trochlea is not a fixed anatomic feature but rather a region whose shape is modulated by the load transmitted across the patellofemoral joint during skeletal growth. Chronic lateral patellar tracking, of the kind imposed by persistent valgus and elevated TT–TG distance, can therefore translate, in the still-developing knee, into a shallow, dome-shaped, or even convex trochlea — exactly the morphology observed here. The result is a self-reinforcing biomechanical loop: malalignment causes maltracking, maltracking remodels the trochlea, the dysplastic trochlea further destabilizes the patella, and the medial patellofemoral ligament is progressively attenuated. By adulthood, the joint may exhibit fixed lateral patellar dislocation, as in our patient, rather than the episodic instability typical of primary trochlear dysplasia.
Fourth, the imaging strategy in such patients should be comprehensive. Standing full-length radiographs are indispensable for quantifying mechanical-axis deviation and identifying the anatomic apex of deformity (CORA analysis). CT remains the standard for measuring TT–TG distance and characterizing trochlear morphology, while MRI assesses the medial patellofemoral ligament, cartilage status, and any associated chondral lesions. From a management standpoint, isolated soft-tissue procedures (e.g., MPFL reconstruction) are unlikely to provide durable stability in the presence of severe bony malalignment; staged correction beginning with realignment osteotomy — potentially combined with tibial tubercle medialization and, where indicated, trochleoplasty — is generally required.
Finally, this case offers a cautionary note on long-term follow-up. Patients with rachitic deformity treated in childhood are frequently discharged from skeletal surveillance once acceptable alignment and growth are achieved. Yet the patellofemoral consequences of residual malalignment may not declare themselves until the second or third decade, by which time the trochlea and extensor mechanism have undergone irreversible adaptive remodeling. Maintaining periodic clinical and radiographic review through skeletal maturity, with a low threshold for cross-sectional imaging when anterior knee symptoms develop, would seem prudent in this population.
Conclusion
Sequelae of childhood rickets can extend well beyond the static deformity visible on plain radiographs. Persistent mechanical-axis deviation, even after corrective osteotomy, may drive the development of secondary trochlear dysplasia, an elevated TT–TG distance, and ultimately fixed lateral patellar dislocation in adulthood. Radiologists encountering an adult with patellofemoral instability and femoral bowing should examine the metaphyses carefully for residual rachitic stigmata and Harris lines, as recognition of the underlying pediatric disease has direct implications for surgical planning and counseling.
Teaching points
- Harris growth-arrest lines and femoral diaphyseal bowing are durable radiographic footprints of childhood rickets that persist into adulthood.
- Distal femoral osteotomy may inadequately correct a deformity whose apex lies in the diaphysis; residual mechanical-axis deviation is common.
- Chronic lateral patellar maltracking during skeletal growth can induce secondary trochlear dysplasia, producing fixed rather than episodic dislocation.
- Comprehensive evaluation of the unstable adult patellofemoral joint with a rachitic background requires standing full-length radiographs, CT (TT–TG, trochlear morphology), and MRI (MPFL, cartilage).

0 COMMENTS
These issues are no comments yet. Write the first comment...