Not Only Bone Breaks: Implant Failure in Atypical Femoral Fracture
Mehmet Fatih Tumer, MD, and Ozgur Tosun, MD
Department of Radiology, Izmir Katip Celebi University, Ataturk Training and Research Hospital, Izmir/Turkey
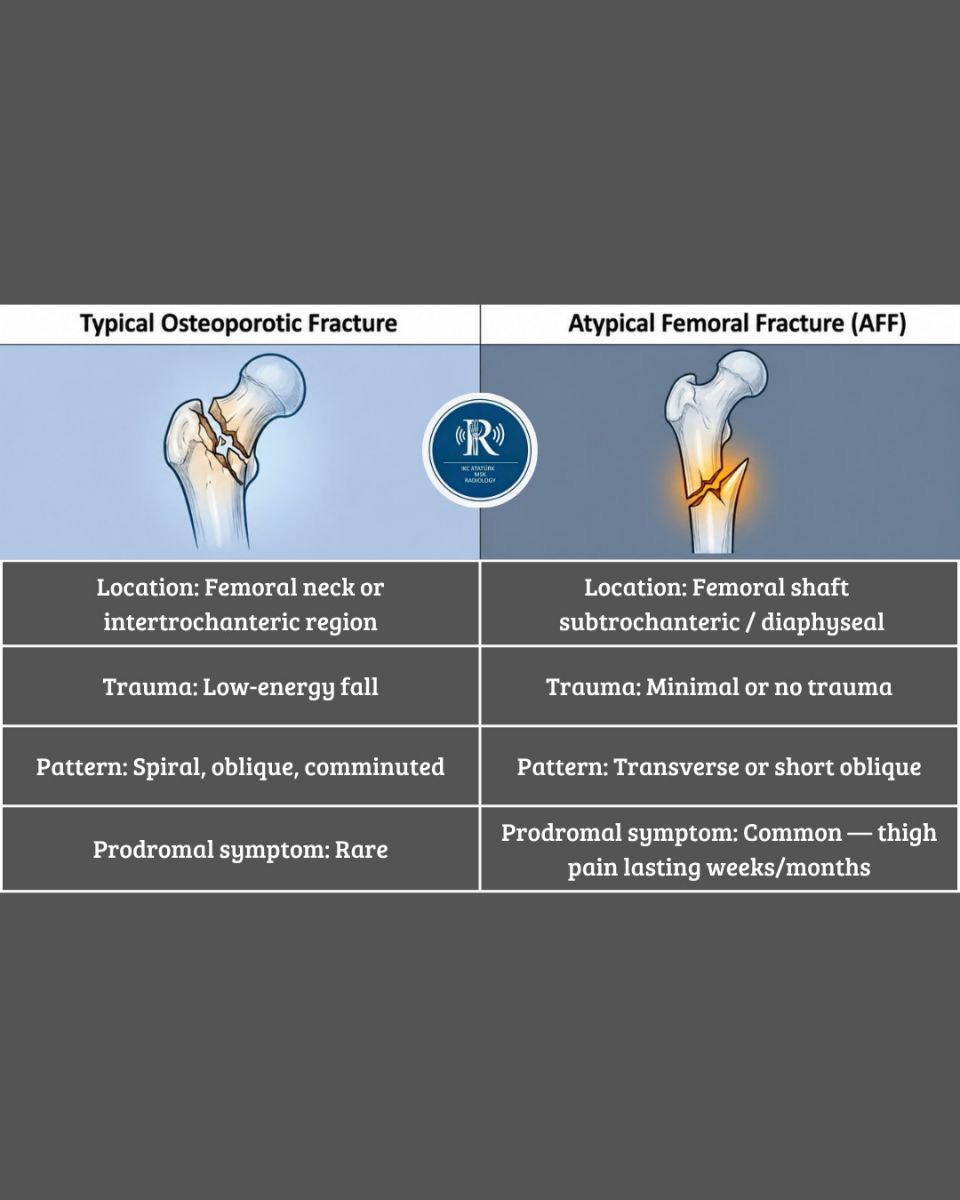
Atypical femoral fractures (AFFs) are distinctive fractures occurring in the subtrochanteric or diaphyseal femur in patients receiving long-term antiresorptive therapy, particularly bisphosphonates or denosumab. These fractures typically occur with minimal or no trauma and exhibit characteristic radiographic features.
The American Society for Bone and Mineral Research (ASBMR) revised its diagnostic criteria in 2014, requiring at least four out of five major criteria for diagnosis.
Pathophysiologically, AFFs result from suppressed bone remodeling due to osteoclast inhibition, leading to accumulation of microdamage, particularly in the lateral femoral cortex, where tensile stress is greatest. Over time, this process evolves from a stress reaction to a complete transverse fracture.
CASE REPORT
Patient History
An 85-year-old woman with postmenopausal osteoporosis diagnosed in 2014 had been treated with antiresorptive agents, predominantly bisphosphonates, for over 11 years. She had no history of diabetes, rheumatologic disease, or long-term corticosteroid use.
Initial Presentation — September 2025
The patient presented with sudden onset of left thigh pain while walking, accompanied by an audible “crack,” without any history of trauma. She reported intermittent prodromal thigh pain over the preceding weeks
Initial Radiological Assessment
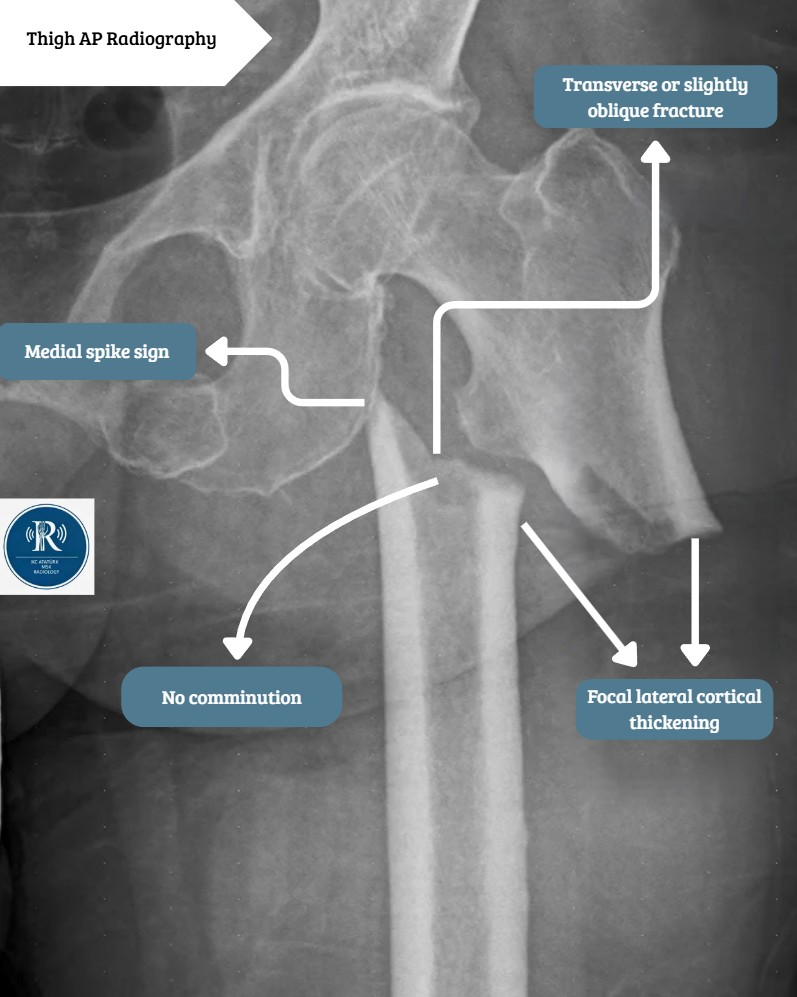
Anteroposterior radiograph of the left femur demonstrated a displaced subtrochanteric fracture.
Four cardinal features supporting AFF were identified
- Focal lateral cortical thickening (“beaking”)
- Transverse/short oblique fracture pattern
- Medial cortical spike sign
- Absence of comminution
These findings, together with the clinical context, fulfilled the ASBMR diagnostic criteria for AFF.
Surgical Treatment
The patient underwent internal fixation with a proximal femoral nail (PFN) and additional plate-screw augmentation. Early postoperative imaging confirmed adequate reduction and fixation.
First Follow-up — November 2025 (2 Months)
Radiographs demonstrated progressive fracture healing, and the patient was clinically asymptomatic.

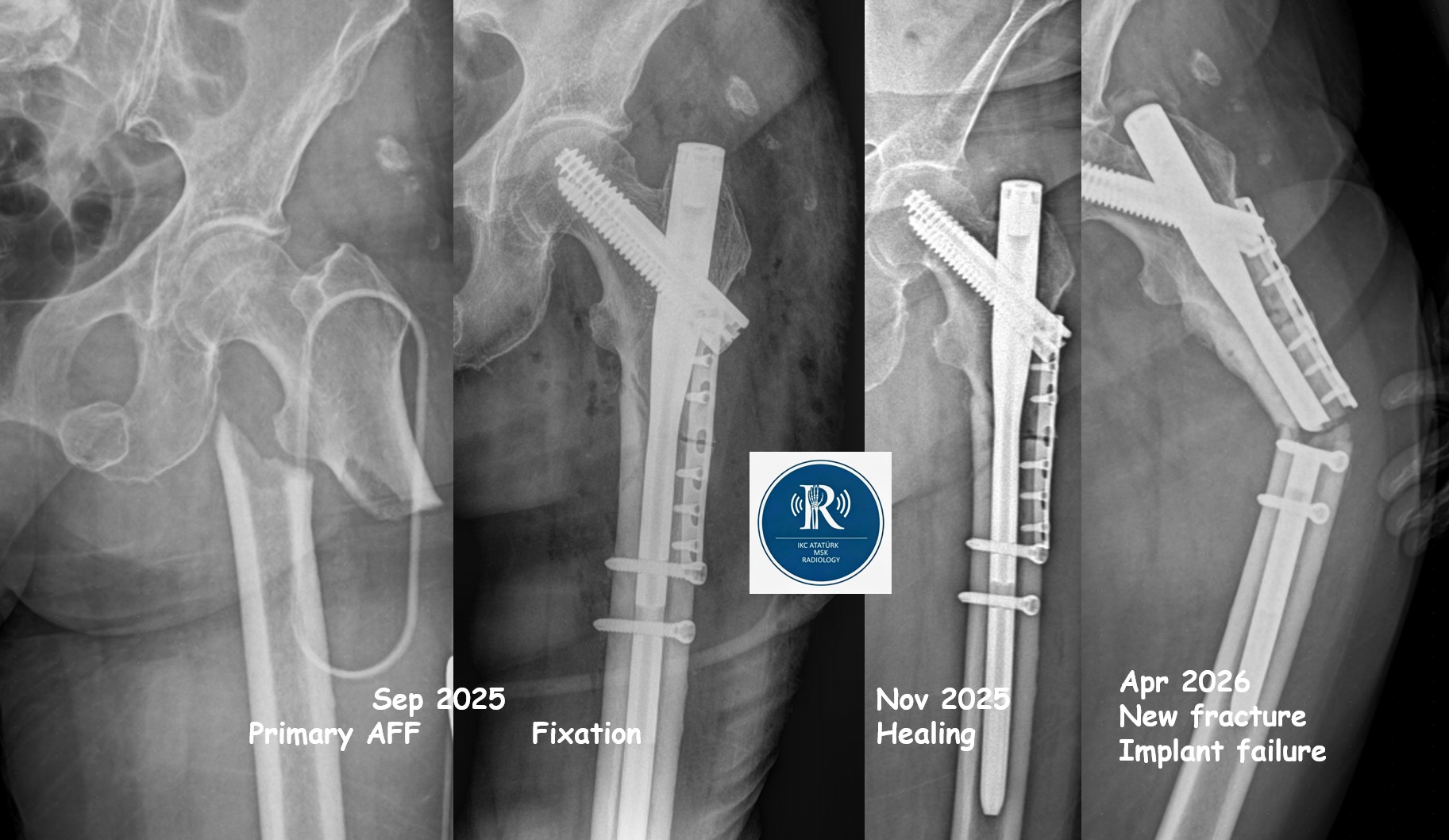
Timeline Summary
As shown in the figure, the radiological course includes:
- September 2025: Primary AFF and fixation
- November 2025: Healing phase
- April 2026: New fracture and implant failure
- Second Presentation — April 2026 (6 Months Postoperative)
- The patient presented again with progressive thigh pain during walking, without trauma
Second Radiological Assessment — New Fracture and Implant Failure
Comparison of 2-month and 6-month postoperative radiographs revealed two critical findings:
- New transverse fracture distal to the healed site
Located in the diaphysis, not bridged by the implant, consistent with a second AFF episode. - Fracture of the femoral implant at the same level
Representing mechanical hardware failure.
This reflects the key principle:
Surgical fixation does not resolve the underlying biological impairment in bone remodeling.
REVISION SURGERY — April 2026
The fractured implant was removed and replaced with a longer intramedullary nail that bridged the entire femur. This strategy redistributes load along the femoral shaft and reduces stress concentration.
DISCUSSION
Pathophysiology of AFF
Bisphosphonates suppress osteoclastic activity, reducing bone turnover. While beneficial in reducing osteoporotic fractures, prolonged use leads to impaired remodeling and accumulation of microdamage, particularly in the lateral cortex. Over time, this results in stress fractures progressing to complete transverse fractures.
Implant Failure — Biomechanical Consequence
Implant failure is a critical yet underrecognized complication in AFF.
Radiological signs include:
- Visible implant fracture
- Screw loosening (periscrew lucency)
- Implant migration
- New fracture lines near stress concentration zones
- Axis deviation or bending
The underlying mechanism is:
Delayed biological healing → prolonged load-bearing by implant → cyclic stress → fatigue failure
Surgical Considerations
- A long intramedullary nail bridging the entire femur is preferred
- Short constructs may leave distal stress risers
- The contralateral femur should always be evaluated
- Medical therapy should be reassessed (e.g., consider anabolic agents)
TEACHING POINTS
- Always question the medication history in atraumatic femoral fractures
- Lateral cortical thickening is the earliest sign
- Medial spike is highly specific for AFF
- AFF is frequently bilateral—image the contralateral femur
- Healed fracture ≠ resolved disease
- Implant failure must be actively evaluated
- Long nail fixation is biomechanically advantageous
- Prodromal pain is a red flag
- ASBMR criteria should guide diagnosis
- AFF requires multidisciplinary management
This case emphasizes that an atypical femoral fracture is not a single radiological event but a dynamic, progressive biomechanical process.
Recognition of the initial fracture is crucial; however, ongoing surveillance is equally important, as new fractures and implant failure may develop.

0 COMMENTS
These issues are no comments yet. Write the first comment...