Tenosynovial Giant Cell Tumor of the Shoulder

Clinical Presentation
A 32-year-old woman presented with chronic left shoulder pain without a history of significant trauma. Physical examination revealed mild pain with active abduction and a palpable fullness in the anterior shoulder region.
Imaging Findings
Modality: Magnetic Resonance Imaging (MRI)
Location: Coracoclavicular space, adjacent to the supraspinatus tendon
Key Imaging Features:
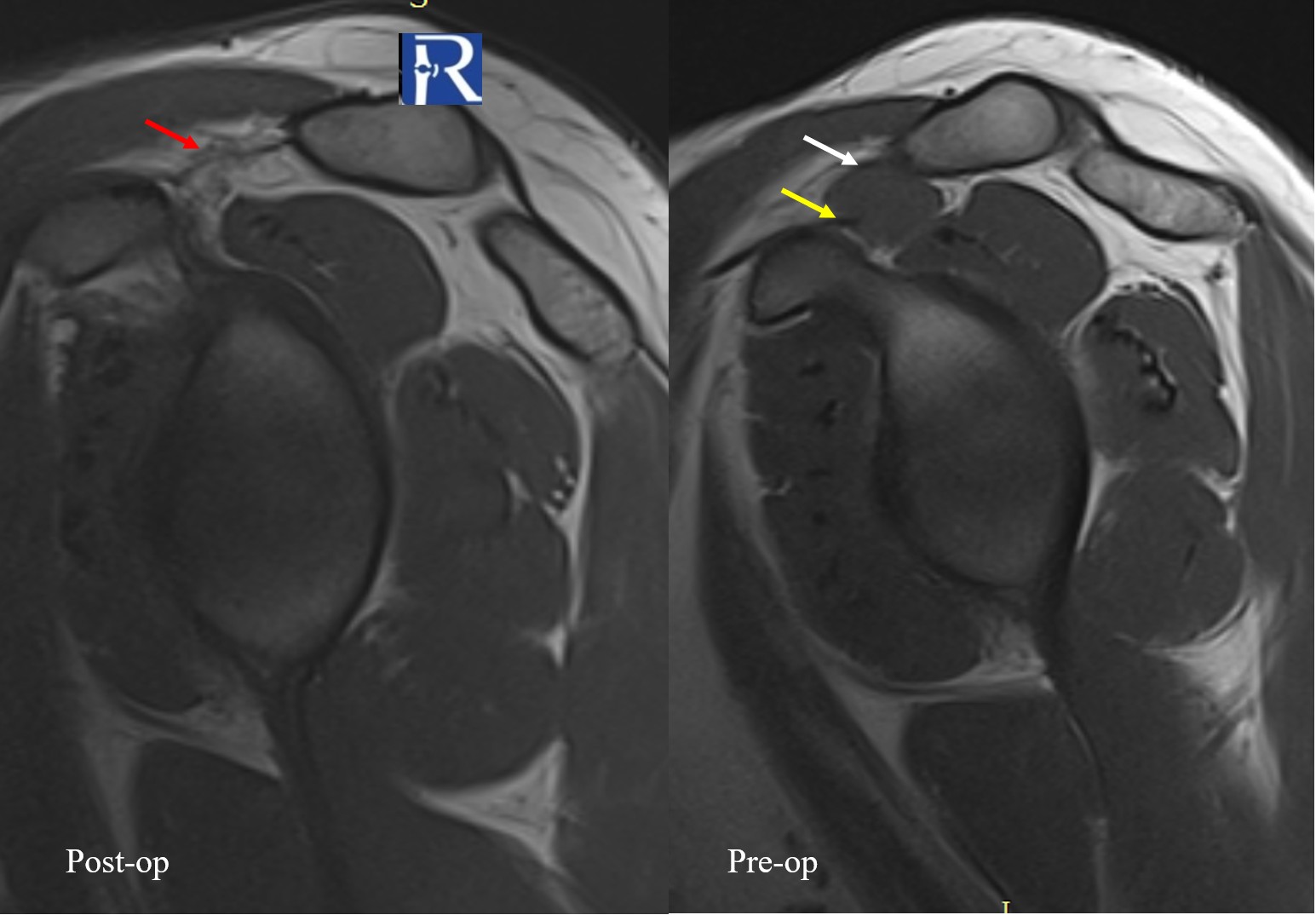
- A well-defined solid soft-tissue mass located between the coracoclavicular and coracoacromial ligaments, immediately adjacent to the supraspinatus musculotendinous unit.
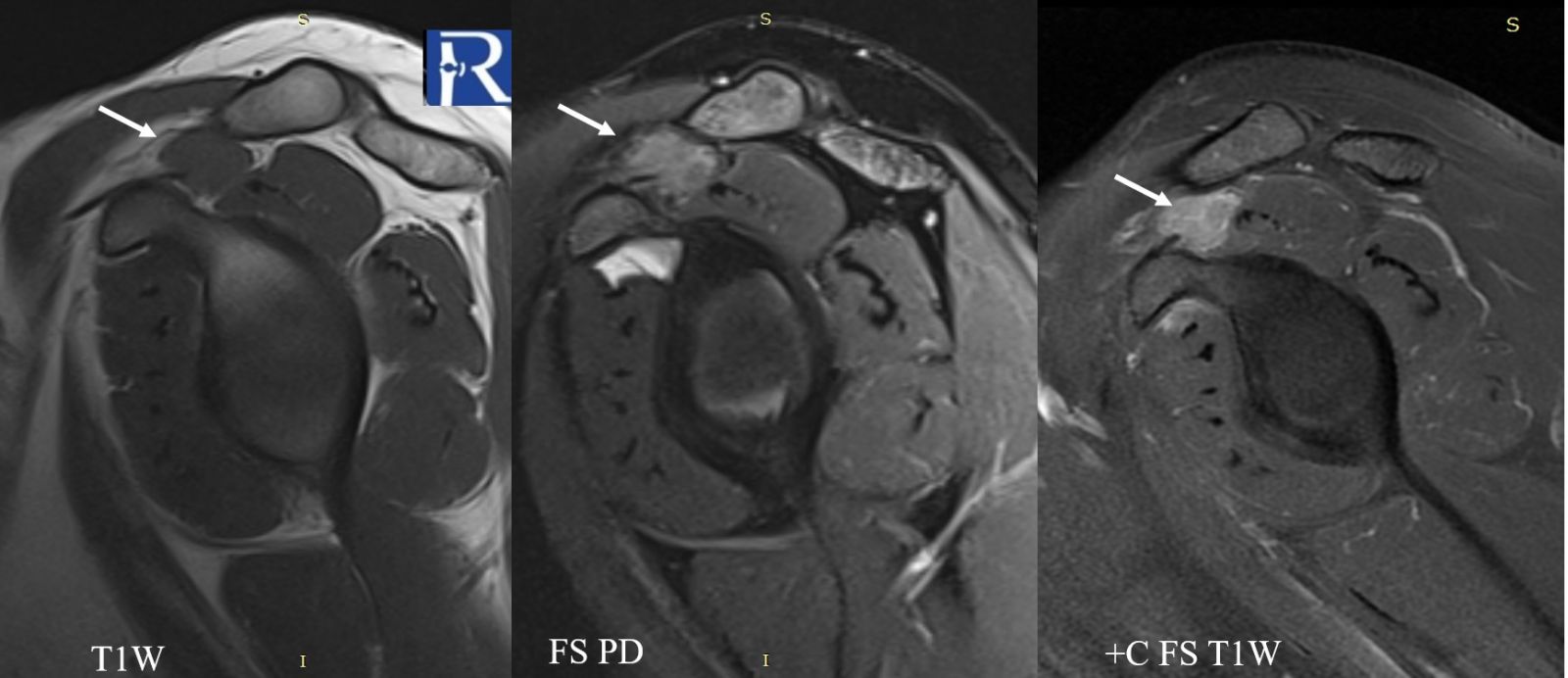
- The lesion is isointense to muscle on T1-weighted images.
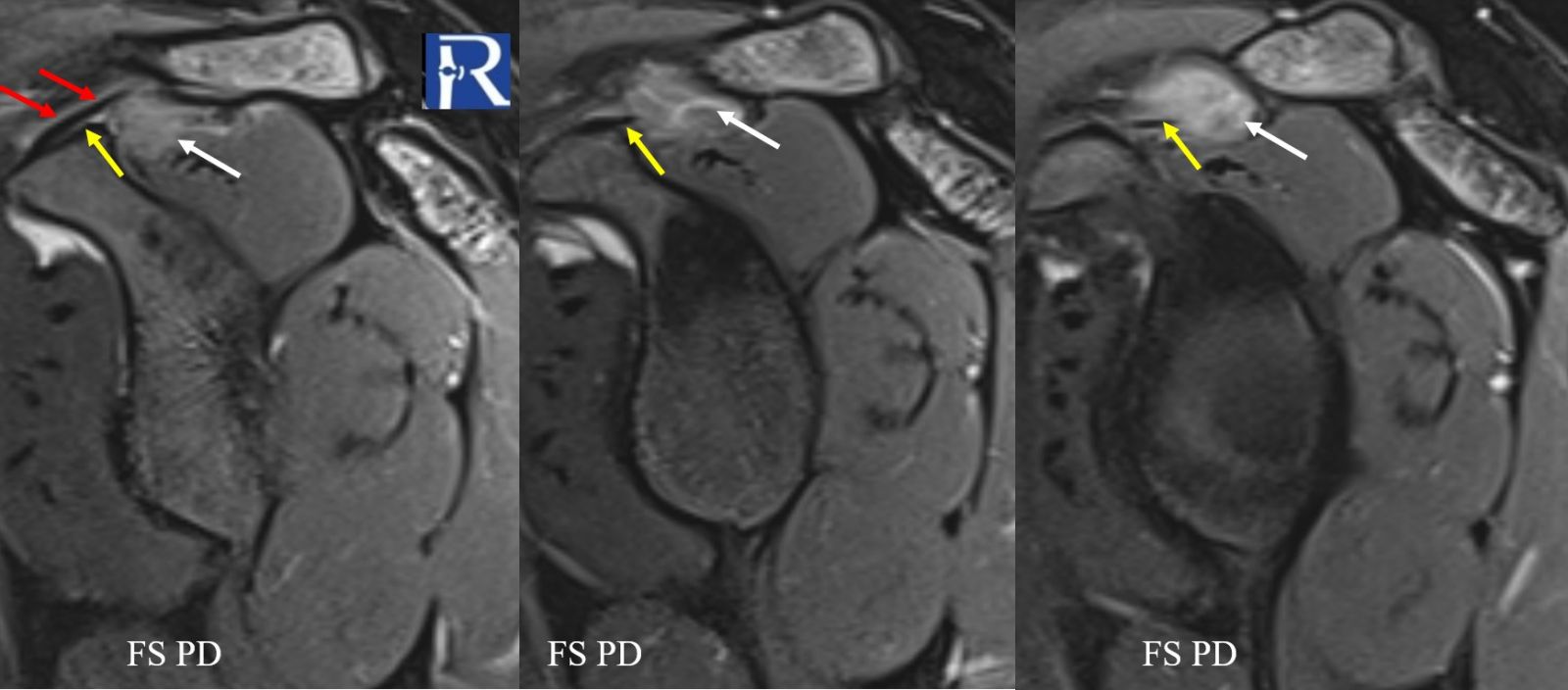
- On fat-suppressed proton density sequences, the mass demonstrates intermediate to low signal intensity.
- Following contrast administration, the lesion shows marked diffuse enhancement.
- On fluid-sensitive (fat-suppressed) sequences, the lesion again exhibits intermediate-to-low signal, suggestive of hemosiderin or cellular lesion.
Imaging Interpretation:
The combination of location adjacent to tendon/synovial structures, signal characteristics, and contrast enhancement pattern raised the suspicion for a tenosynovial giant cell tumor (TGCT).
Differential Diagnosis
The imaging appearance of a soft-tissue mass with intermediate to low signal on fluid-sensitive sequences and proximity to tendon structures should prompt consideration of:
- Tenosynovial Giant Cell Tumor (TGCT)
- Synovial sarcoma
- Nodular fasciitis
- Ganglion Cyst
- Pigmented villonodular synovitis (historically used, not recommended per 2020 WHO)
Pathology
The patient underwent surgical excision of the lesion.
Histopathological examination was consistent with a Tenosynovial Giant Cell Tumor (formerly referred to as a localized type of pigmented villonodular lesion), confirming the imaging diagnosis.
Diagnosis
Tenosynovial Giant Cell Tumor (Localized Type)
Discussion
Tenosynovial Giant Cell Tumors (TGCTs) are benign, fibrohistocytic lesions arising from the synovium of joints, bursae, or tendon sheaths. They belong to a spectrum of tumors showing synovial differentiation.
Epidemiology:
- Most frequently affect individuals aged 30–50 years
- Slight female predominance (female:male ratio ~1.5–2.1:1)
Anatomic Distribution:
- Localized TGCTs are most commonly seen in the fingers, adjacent to tendon sheaths and interphalangeal joints (~85% of cases).
- Less commonly, they occur in the wrist, ankle, foot, and knee.
- Very rarely, lesions are identified in the elbow and hip.
Terminology:
- Previously described as pigmented villonodular tumor of tendon sheath (PVNTS) or localized/focal nodular synovitis.
- Per 2020 WHO Classification, the term pigmented villonodular synovitis (PVNS) is no longer recommended for localized soft-tissue lesions.
MRI Characteristics:
- Well-circumscribed, nodular soft-tissue mass
- Intermediate to low signal on T1 and T2 sequences
- Variable hemosiderin content may cause focal low signal areas
- Enhancement after contrast is typical
- Relationship to tendon sheath/synovium is an important clue
Teaching Points:
- TGCT should be included in the differential diagnosis of soft-tissue masses adjacent to tendon or synovial structures, especially in the appropriate age group.
- Recognition of low signal on fluid-sensitive sequences and enhancement pattern assists in differentiating TGCT from other soft-tissue tumors.
- Histopathological confirmation remains the gold standard.

0 COMMENTS
These issues are no comments yet. Write the first comment...