Arcuate Sign (Knee): Fibular Head Avulsion & Posterolateral Corner Injury

The arcuate sign is a fibular head avulsion fracture indicating posterolateral corner injury, commonly associated with ACL and PCL tears. Early recognition on X-ray and MRI is crucial.
Clinical context:
A 52-year-old male presented with knee pain and instability following a fall from approximately 2 meters, a mechanism consistent with high-energy trauma. Such injury patterns should immediately raise suspicion for complex ligamentous damage, particularly involving the posterolateral structures of the knee.
Radiographic findings:
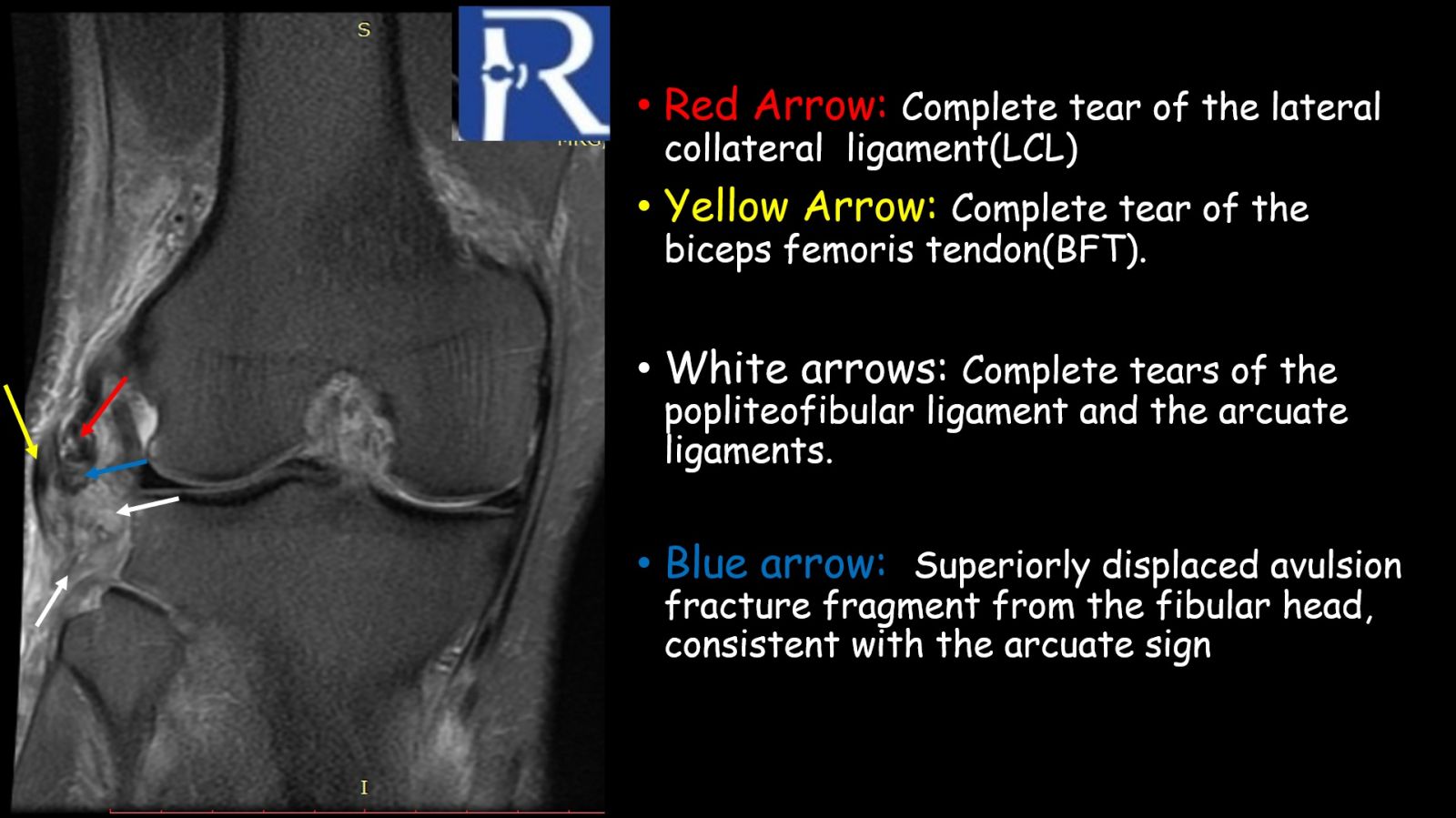
Plain radiographs demonstrated a superiorly displaced avulsion fracture of the fibular head, consistent with the arcuate sign. Although often subtle, this finding represents an avulsion at the insertion site of the arcuate ligament complex and is a well-recognized radiographic marker of posterolateral corner (PLC) injury. The fracture fragment is typically attached to the fibular (lateral) collateral ligament, the biceps femoris tendon, or both, and its size and displacement pattern may vary depending on the injured structure.
.jpeg)
MRI findings:
MRI confirmed a superiorly displaced avulsion fragment arising from the proximal fibula and provided comprehensive evaluation of associated soft tissue injuries. There was extensive involvement of the posterolateral corner, including a full-thickness tear of the biceps femoris tendon, disruption at the LCL/conjoined tendon insertion, and a high-grade partial tear of the popliteus tendon at its femoral attachment.
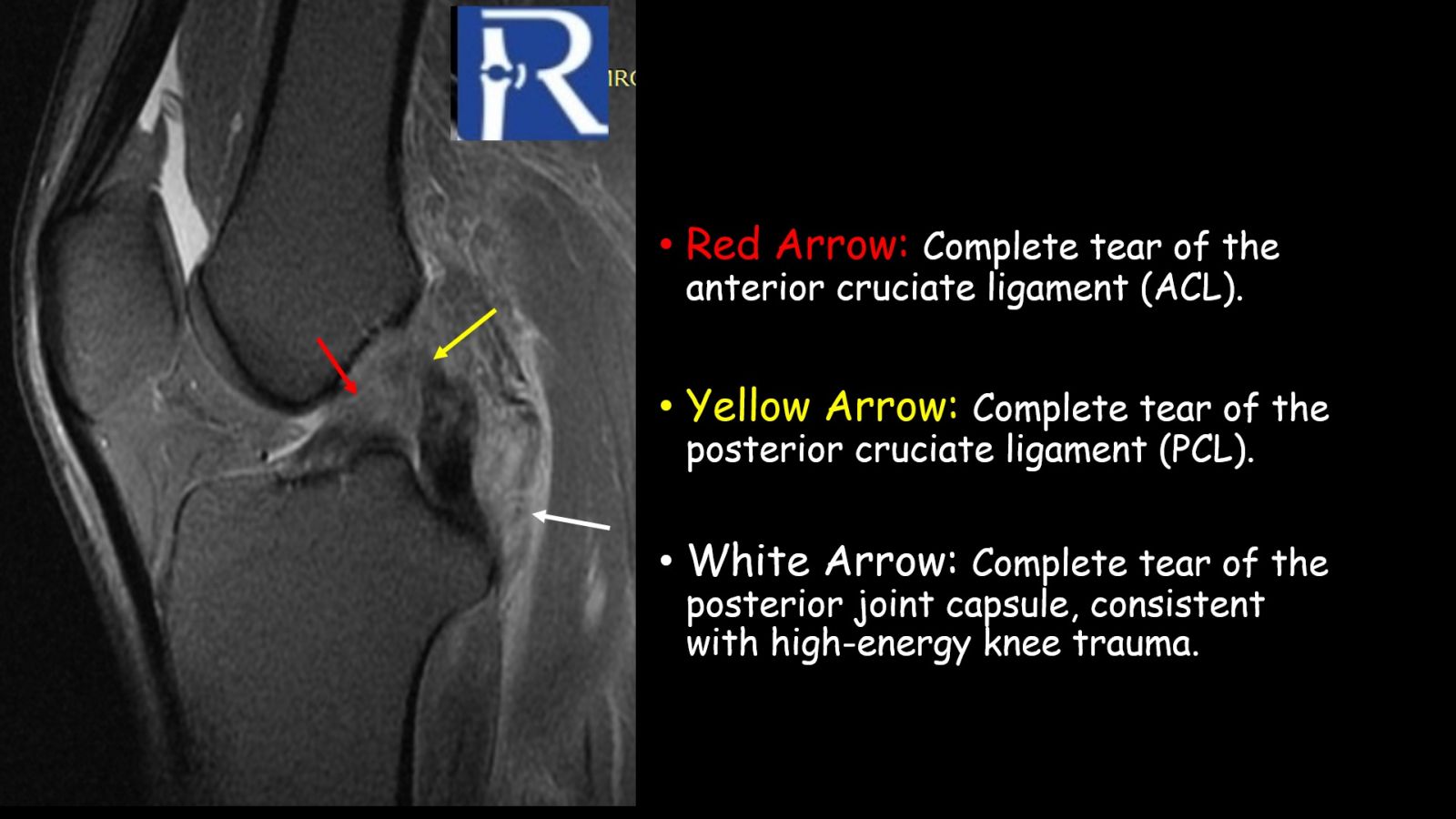
Cruciate ligament injuries were also present, with a complete tear of the anterior cruciate ligament (ACL) and a near–full-thickness high-grade partial tear of the proximal posterior cruciate ligament (PCL). Additional associated findings included a high-grade partial tear of the lateral retinaculum, strain-related signal changes in the medial retinaculum and medial collateral ligament, and edema-like signal along the common peroneal nerve. The menisci, patellofemoral alignment, patellar cartilage, and extensor mechanism were otherwise preserved.
.jpeg)
Mechanism and imaging correlation:
The arcuate sign most commonly results from a direct blow to the anteromedial tibia with the knee in extension, leading to posterolateral subluxation of the tibia in external rotation. An alternative mechanism is sudden knee hyperextension with internal tibial rotation. These mechanisms explain the frequent association with cruciate ligament injuries, reported in up to 90% of cases, particularly involving the PCL.
Why recognition matters:
Failure to identify the arcuate sign in the acute setting may lead to unrecognized posterolateral instability, which is notoriously difficult to treat and is a well-known cause of failed cruciate ligament reconstruction. Importantly, the presence of the arcuate sign should also prompt consideration of a spontaneously reduced knee dislocation, especially in high-energy trauma, and mandates careful evaluation for neurovascular injury, particularly involving the common peroneal nerve and popliteal artery.
Differential diagnosis:
The primary imaging differential diagnosis is a Segond fracture, which differs by originating from the lateral tibial plateau, with the fracture fragment located more anteriorly and medially, rather than from the fibular head.
Key teaching points:
- The arcuate sign is a highly specific marker of posterolateral corner injury
- It is frequently associated with ACL and/or PCL tears
- Its detection should trigger a systematic search for ligamentous, neurologic, and vascular injuries
- A seemingly small avulsion fracture may represent a severe internal derangement of the knee

0 COMMENTS
These issues are no comments yet. Write the first comment...