Meniscal Tears – Comprehensive MRI Guide

Meniscal tears are among the most common knee pathologies encountered in musculoskeletal radiology, arising from trauma, sports injuries, degenerative changes, or altered load transmission within the tibiofemoral joint. Because of their clinical impact, accurate MRI interpretation is crucial in determining tear morphology, evaluating stability, and guiding treatment decisions. Understanding the detailed anatomy of the meniscus—including circumferential and radial collagen fibers, meniscocapsular attachments, and root insertions—is essential, as disruption of these structures profoundly affects knee biomechanics and accelerates joint degeneration. MRI remains the gold standard for diagnosing meniscal tears, offering high sensitivity for characterizing both subtle and complex lesions.
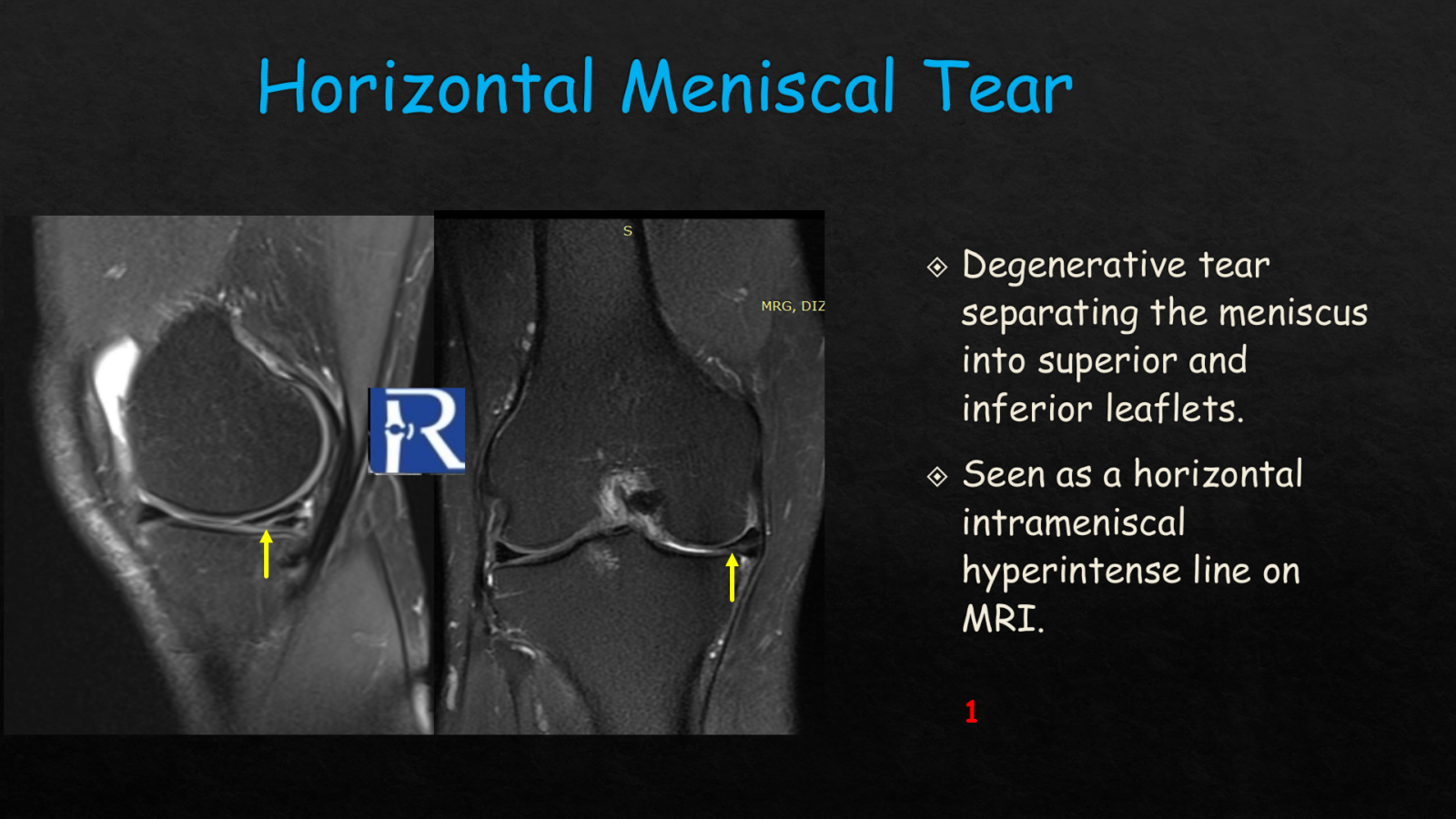
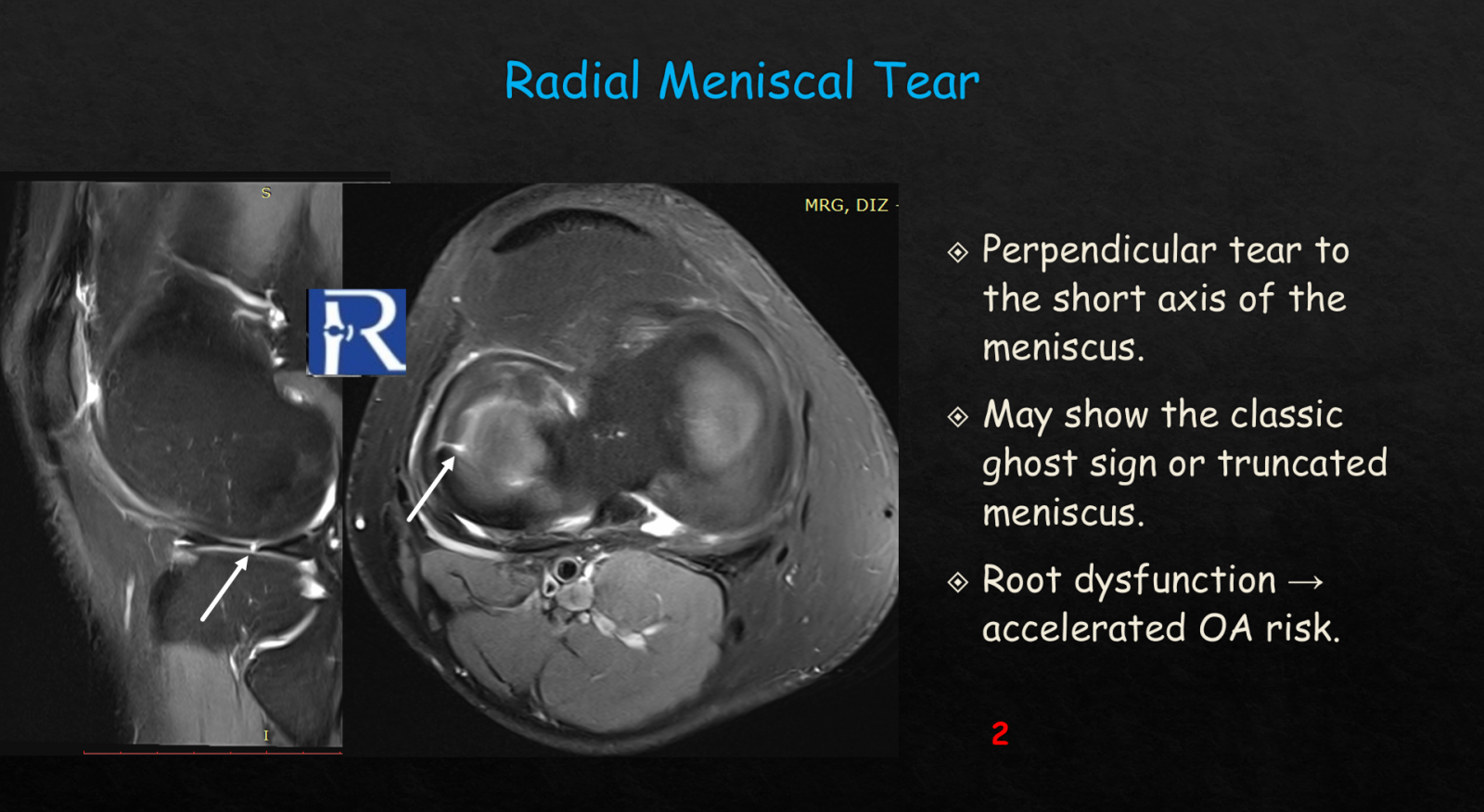
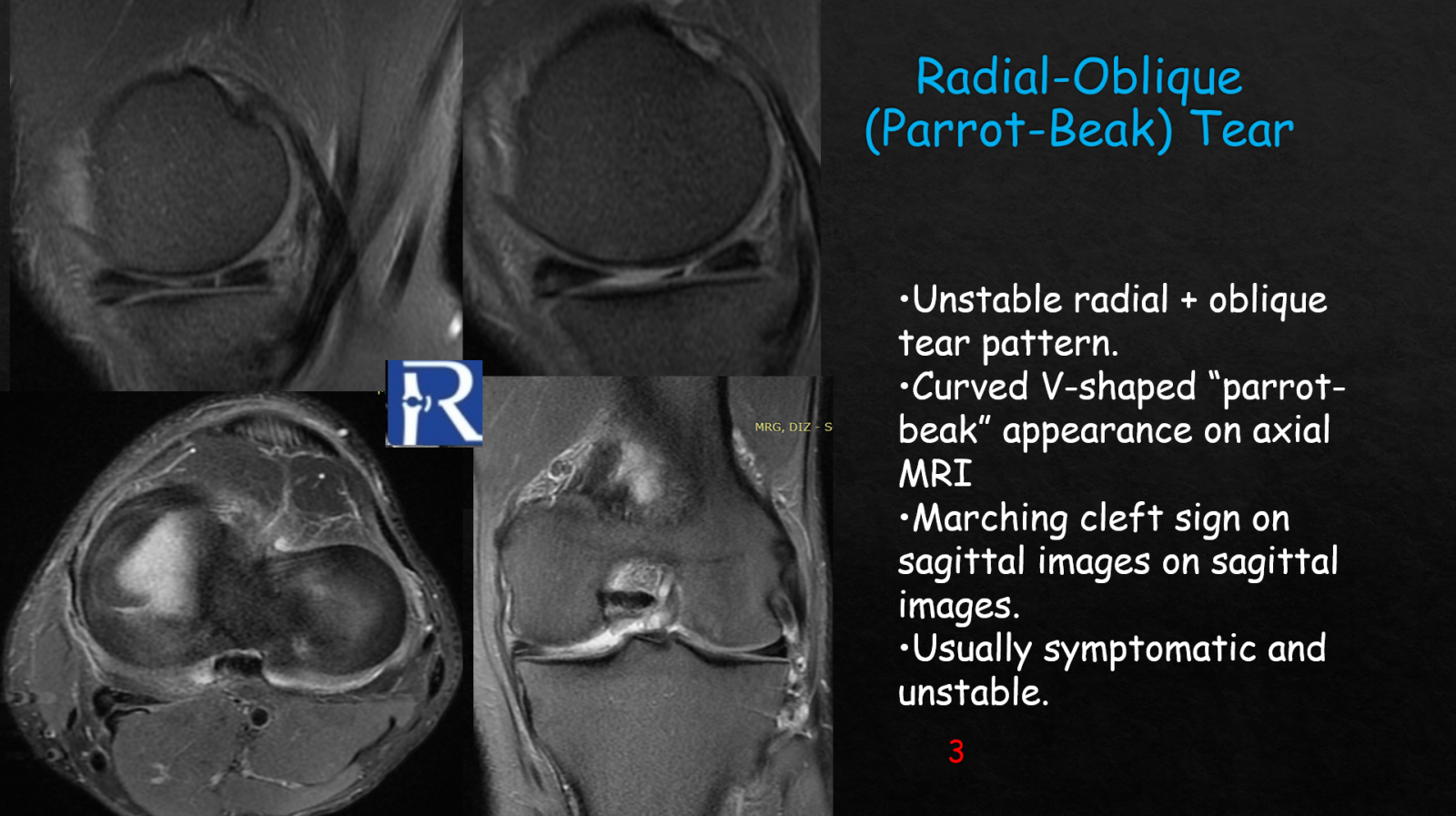
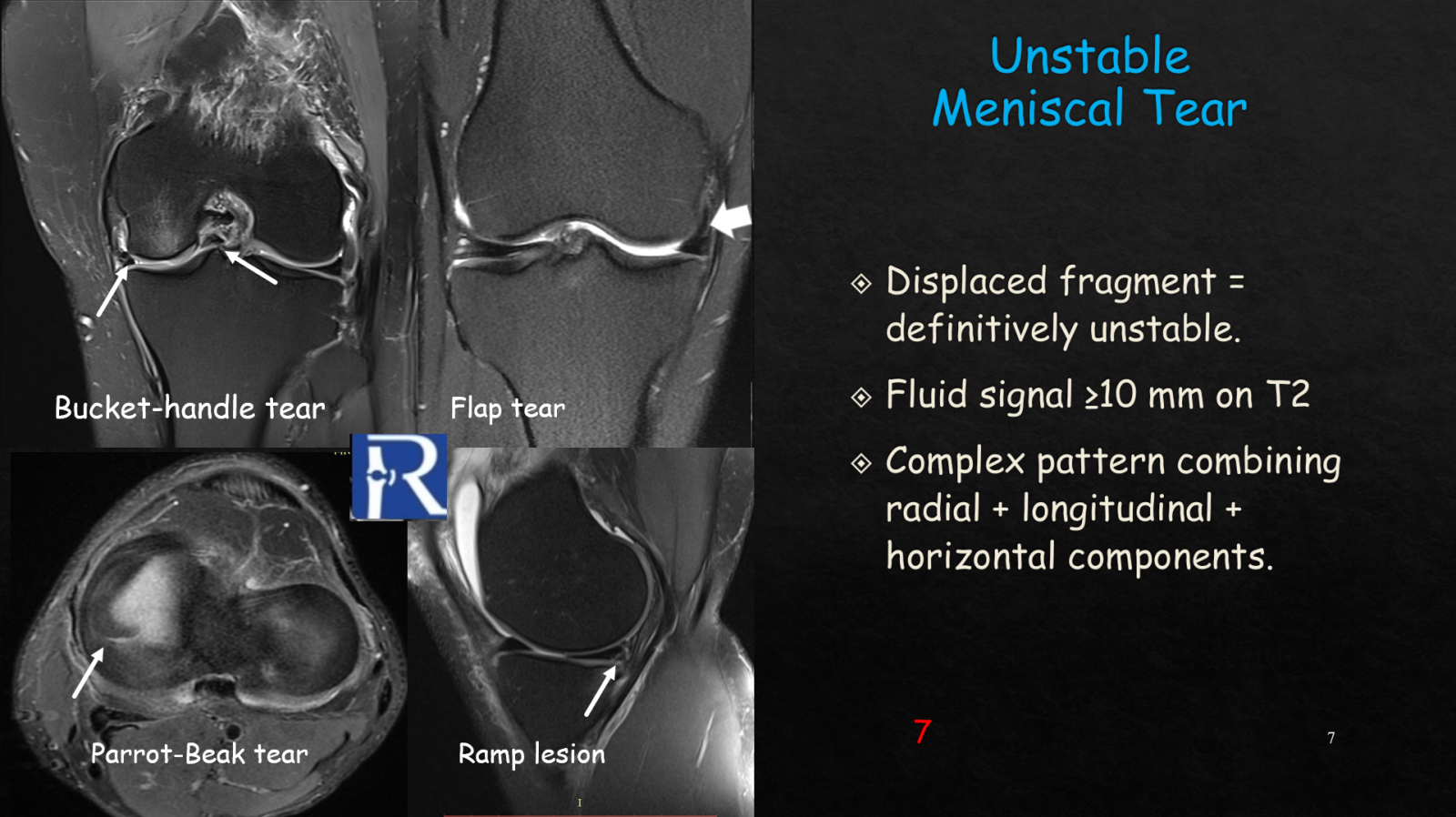
Horizontal meniscal tears, which are commonly degenerative, separate the meniscus into superior and inferior leaflets and appear on MRI as horizontal intrameniscal hyperintense lines, best visualized on proton-density or T2-weighted sagittal sequences. Although often stable, they may occasionally lead to parameniscal cysts or mechanical symptoms. Radial tears are significant because they run perpendicular to the meniscal short axis, disrupting hoop stress mechanics. Their characteristic MRI features include the ghost sign or truncated meniscus appearance, and radial tears near the root are especially concerning due to their strong association with accelerated osteoarthritis. Radial-oblique or parrot-beak tears combine radial and oblique components and form unstable flap configurations. They typically demonstrate a curved V-shaped morphology on axial MRI and sequential clefts on sagittal images, often producing significant mechanical symptoms that require arthroscopic treatment.
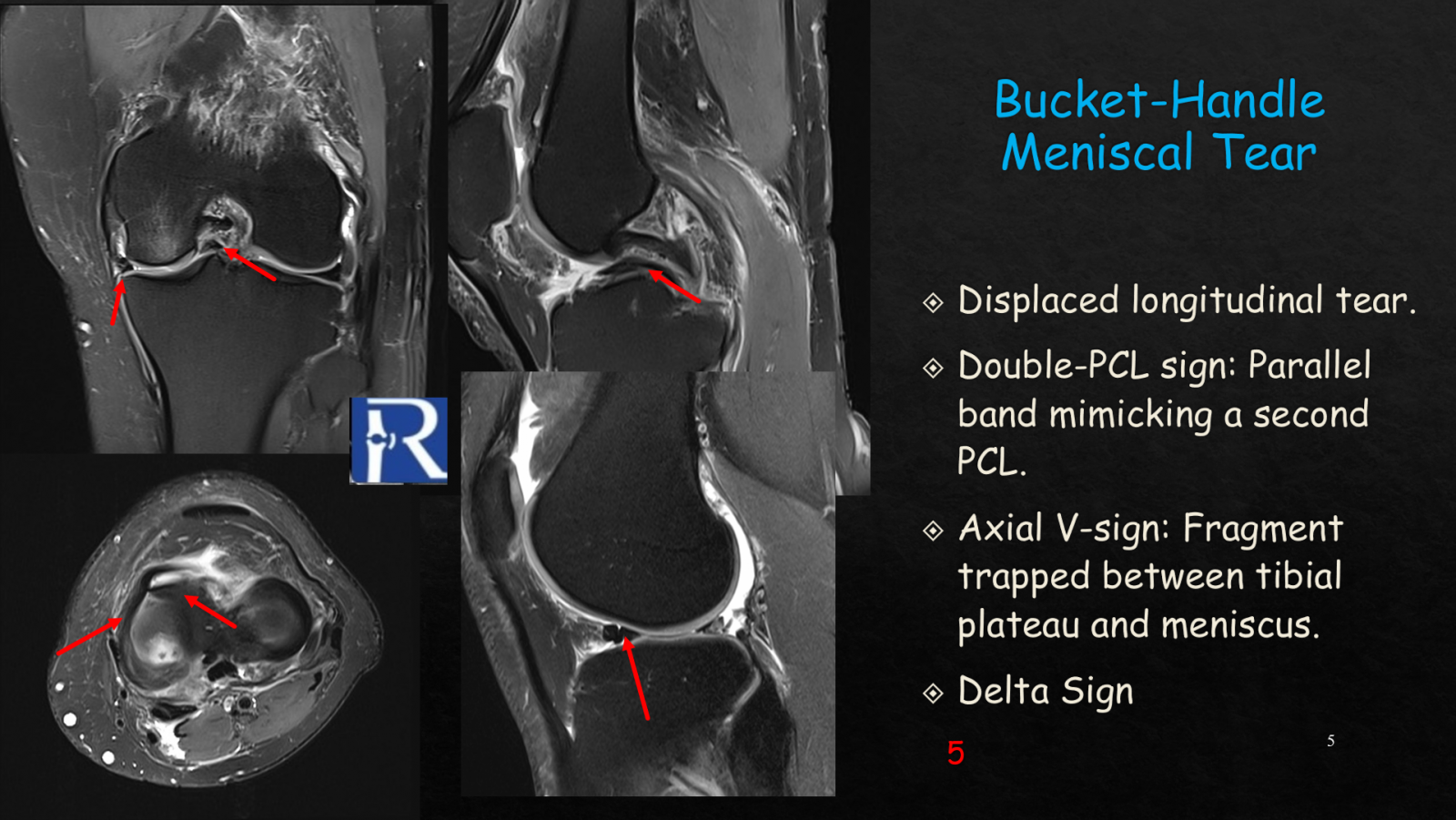
Ramp lesions involve meniscocapsular separation at the medial posterior horn and are commonly associated with ACL tears. They may contribute to persistent rotational instability if overlooked. MRI findings include a T2 hyperintense line between the posterior horn and capsule and posteromedial tibial plateau edema. Bucket-handle tears, one of the most dramatic forms of meniscal injury, involve a displaced longitudinal fragment that flips into the intercondylar notch. These tears are identified using well-known MRI signs, including the double-PCL sign (a fragment parallel to the posterior cruciate ligament), the axial V-sign, and the double-delta sign. These injuries often cause true mechanical locking and require urgent surgical attention.
Flap tears occur when a portion of the meniscus detaches and migrates into the superior or inferior joint recesses. These unstable fragments can mimic loose bodies or chondral fragments and typically produce symptoms such as catching and locking. They often necessitate surgical intervention due to their unstable nature. More complex or unstable meniscal tears exhibit multidirectional tear patterns—combining radial, horizontal, and longitudinal components—with at least 10 mm of fluid signal along the tear or evidence of fragment displacement. These tears are frequently associated with ligamentous injuries and require thorough assessment before treatment.
Early detection of instability and precise classification of tear morphology are essential for optimizing clinical outcomes and tailoring patient-specific treatment strategies. Missed findings, such as small radial tears near the root or subtle ramp lesions, can significantly impact knee biomechanics and long-term joint health. MRI’s ability to distinguish stable from unstable tears, detect associated injuries, and define tear complexity makes it the cornerstone of meniscal pathology evaluation.
By understanding the imaging characteristics of horizontal tears, radial tears, parrot-beak tears, ramp lesions, bucket-handle injuries, flap tears, and unstable complex patterns, clinicians and radiologists can improve diagnostic accuracy and support better surgical planning and patient outcomes. This comprehensive approach ensures that meniscal tear evaluation remains a critical component of knee MRI interpretation and musculoskeletal imaging practice
.png)


0 COMMENTS
These issues are no comments yet. Write the first comment...